Cowper’s Cut 369: The NHS vibes of Wes Streeting

I’m not sure whether Wes Streeting is familiar with the Financial Times columnist and George Osborne biographer Janan Ganesh.
I imagine that he is: both men are articulate, plausible post-Blairite Bright Young(ish) Things, and were or are widely perceived as adornments of the Westminster media scene.
I was set to wondering about this by one of Ganesh’s better FT columns, on the importance of political ‘vibes’.
Ganesh writes that “most people’s ideological commitments are extraordinarily soft. What they think of as a belief is often a post-hoc rationalisation of a group loyalty. Crucially, this is more true, not less, of degree-holding, “high-information” voters. What education can do is estrange people from parents and home town. It leaves them casting around for an alternative identity. Political tribe is as good as any”.
It is an important point that in our political and social age of greater tribalism and lower self-reflection, both politicians and political observers are highly susceptible to the ‘vibes’ of an individual or an argument.
It also creates a real problem for Mr Streeting and his team, because his ‘vibes’ towards the NHS are absolutely fucking terrible.
This matters, because it is likely to make Mr Streeting’s plans for NHS reform (assuming that they ever develop) harder to implement. On the subject of Mr Streeting’s NHS plans, I recommend the comments of Nick Timmins and Siva Anandaciva to the Commons Health Select Committee’s evidence session this week.
Which (assuming that Mr Streeting’s yet-to-emerge plans are any good) is A Bad Thing.
NHS simpering is obviously bad
I do not say this as a fan-boy of the NHS, or as somebody who enjoys the over-familiar broadcast modes of NHS narcissism or NHS simpering. As long-time readers know, I find both of those positions to be as useless as they are nauseating.
The NHS is a near-monopsony single-payer tax-funded system to plan, ration and deliver our healthcare. As such, it is potentially efficient and equitable.
At its best, its staff can be fierce innovators - as seen during the early period of the Covid19 pandemic. Once people can gain access to its A&E services, they remain generally very high-class. Primary care, despite years of resource and workforce retreat, has successfully been doing much more with less - although despite this, patient demand still outstrips supply.
The NHS is also capable of Gandhi-esque passive resistance to patient-centred change (as on electronic patient records); has such negative tribalism both within the clinical tribes and between the clinical and administrative tribes that it needs a Chief Anthropologist far more than it needs any Chief Inspector; and has no discernible means of improving appalling clinical practice in midwifery and mental health services. It lacks scale-able national improvement mechanisms; and its quality and safety regulatory system has been broken for years.
Oh, and unlike most other European health systems, it almost breaks for four months every winter, due to a lack of planning and resources to build in resilience.
There is, in other words, a fair and balanced critique of the NHS to be made.
The problem is that on top of his years as opposition spokesman, Mr Streeting now has a nine-month long history in office of failing to make such a critique. He just shouts ‘reform and modernise!’ at the NHS occasionally.
We have seen his particularly abrupt U-turns on the dissolution of NHS England, but as I wrote just before the General Election last year, the Government was elected with no actual health policy: “Ah well. They will learn the hard way, it seems”.
Preaching to the unconvertible

Among Mr Streeting’s most curious and least endearing qualities is a tendency to preach to the unconvertible: once again glaringly on show in his comment piece for The Times this week. It is a quite startlingly bad piece.
Its opening assertion that “running a department with a budget larger than the government of Portugal, I bear particular responsibility for keeping taxes low, by keeping healthcare costs down” is remarkably silly. The level of welfare spending is evidently pertinent to taxation: so what is the single biggest element of welfare spending?
It is the state pension. It is not the NHS.
Does this piece get any better?
Dear readers, it does not, with its claim that the 2024 Darzi Review “found the NHS has increased labour relative to capital, while every other industry has improved productivity by doing the opposite. To correct that, the chancellor invested more than £13 billion in health and care capital at the budget, to arm the NHS with the equipment, modern technology and buildings it needs.”

Mmmmmmmm. It is hard to like this when even on the SOS’s and Chancellor’s watch, the longstanding, grim tradition of capital-to-revenue transfers continued.
Nor does the bullshit stop with his subsequent assertion that “alongside that investment, our reform agenda is cutting out wasteful practices. Where technological and medical advancements have been made over the past decade, the NHS has failed to realise the benefits.
“Ten years ago, a patient going into hospital for a procedure would stay there for several days afterwards to recover. With a growing number of surgeries, patients can now go home later the same day. For some procedures, patients no longer need to go into hospital at all.
“These innovations are better for the patient, and less expensive for the NHS. By lowering the tariff hospitals are paid for these procedures, we will force the NHS to modernise, just one area where this government is changing things to get more bang for taxpayers’ buck.”
This argument is straightforwardly nonsense, as the Getting It Right First Time work (easily found through an internet search) demonstrates. As it states, “data from March - May 2024 shows that 83.9% of surgical procedures in the BADS Directory of Procedures within England are being undertaken as day cases or outpatient procedures (Model Health System), just shy of the 85%1 expectation, with large variation between providers.”
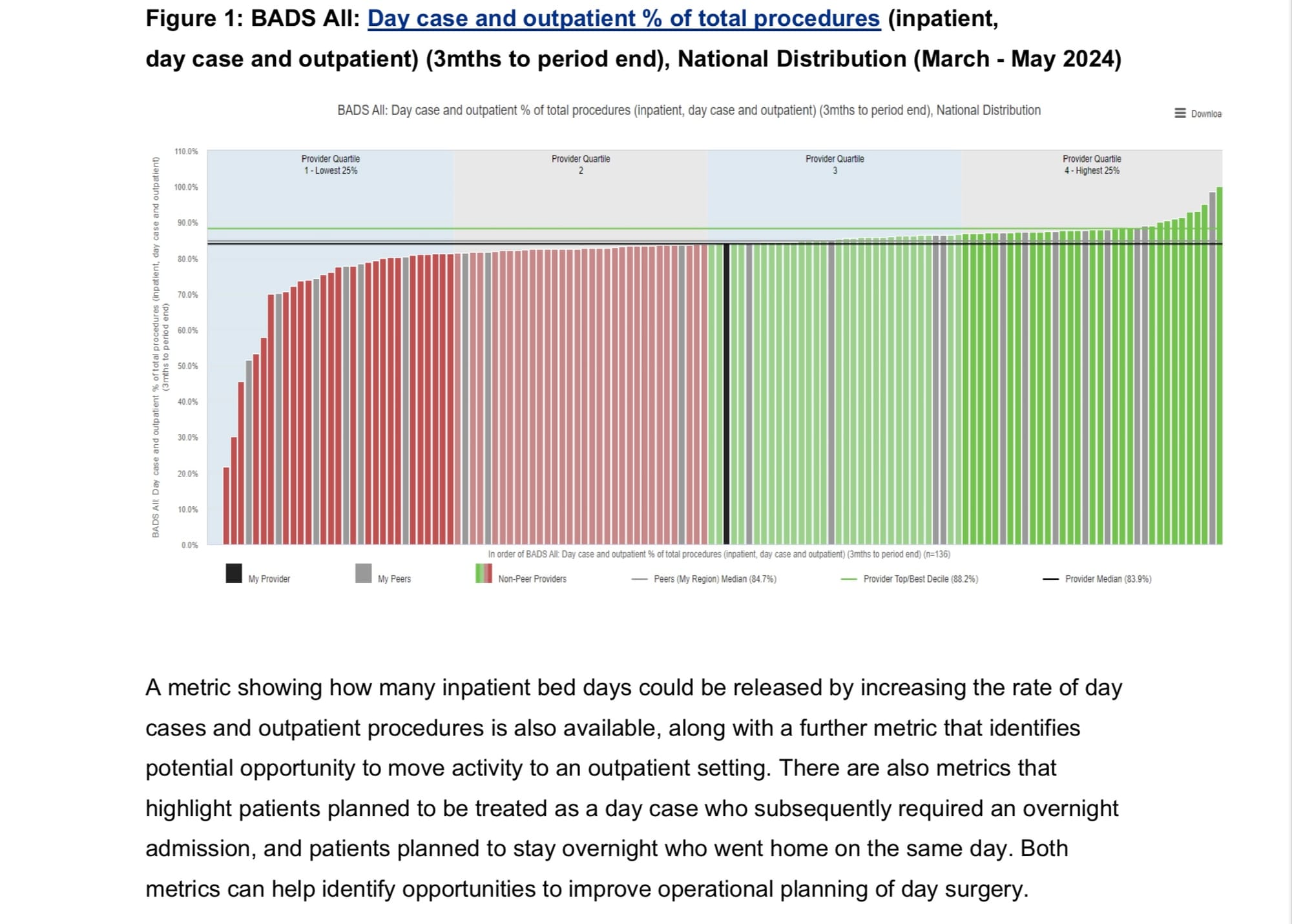
Look at the report’s own graph of the data, above. This is not a serious national problem, other than at the lowest-performing margins.
There is a small amount of not-absurd content on staffing agency rates, but then we are back to nonsense with “the good news is that, starting from such a low base, there is huge potential to transform patients’ care at vastly greater value for taxpayers’ money, by going further and faster on NHS productivity.
“If every NHS trust was as efficient as the top performers, it would be equivalent to an extra £20 billion, without having to raise a penny in tax. New league tables will soon hold providers properly to account, with incentives and tough interventions to lift up the laggards.
“The abolition of NHS England will halve headcount and end wasteful duplication, and I will shortly be setting our further reforms to drive costs down and productivity up.”
In the absence of any demonstrable theory of change - a means to help or drive every NHS trust to be as efficient as the top performers (a topic that has been of remarkable disinterest to any part of senior English NHS national or political leadership) - this is just pathetic rhetoric.
The article’s sole reform idea? League tables. Ah yes, we had those: why were they abolished?
Oh, the Mid-Staffs Public Inquiry, that’s why.
Pre-‘Not A Budget, Honest’ tanks on lawns for social care funding?

Wes Streeting seems to have remembered the ‘But Social Care’ bit in his job title this week, conveniently just a few days before Chancellor Rachel Reeves’ Spring Statement. He told BBC Panorama that “I want to spend more of our resources through social care because it delivers better outcomes for patients and better value for taxpayers. So I’m convinced that we can spend NHS resources more effectively through social care ... the 10-year plan for health will include elements of social care, because the two do have to go hand in hand together.”
Streeting also repeated his belief that the NHS is “also not all about money: you can’t just keep on pouring ever increasing amounts of taxpayers’ money into a system that is not set up to deliver best use of that money and best care for patients and that’s why the system needs to change”.
What comes next?
It’s becoming increasingly apparent that integrated care boards and systems have had their not-much-of-a day.

This week, NHS England’s new draft Performance Assessment Framework was spotted by Health Service Journal’s Mimi Launder. It promises to “reduce duplication and prevent providers from being bombarded with conflicting instructions”, including by removing integrated care boards’ performance management role.
The document confirms that NHSE, not ICBs, will be responsible for provider performance management: “discussions about performance will be led by colleagues at NHS England, who are experienced in addressing delivery challenges.”
Provider trusts’ performance “segments” will no longer take into account wider system performance, nor a proposed judgement of their “capability”, as they will “solely [be] linked to delivery metrics”. Targets are back, baby!
Yet apparently, ICBs will still be expected to “hold their partners to account using the system levers that bind them together, such as their joint system plans, partnership agreements, joint committees and collaboratives”.
Mmmmmm. Good luck with doing that, with no resources.
So integrated care is no longer A Thing. This is a pragmatic recognition of both Labour’s manifesto commitment to re-achieving 18 weeks RTT by 2029 and doing its best on A&E; as well as of the reality of ICBs’ cumulative 80% management cuts.

This point was also cogently made in former NHS Commissioning Board chief executive Sir David Nicholson’s statements that ICBs will have to merge, also in HSJ.
The likely fate of ICBs is to be aggregated up into the new regions or strategic health authorities, together with whatever is allowed to remain of NHS England’s regional presences.
Another leak to HSJ (which must currently be inundated with such) revealed that NHS England hopes to tackle “a perceived devaluing of commissioning” and enhance “the skills and professional identity of commissioners”, as part of ICBs’ future.
That’s a curious idea, because as they were originally conceived, ICBs evidently haven’t got a future.
The leaked slides outlining NHSE’s plans sent to HSJ, say, “there has been a perceived devaluing of commissioning and a consequent variation in capability and capacity to carry it out across health economies.”
It must now, it says “set out what commissioning means now, building the skills and professional identity of commissioners to meet the challenges but also the opportunities afforded in 2025”.
I think we can help them with that.
Commissioning now means nothing - or put slightly differently, it means whatever Wes Streeting wants it to mean.
And what Wes Streeting (or perhaps more accurately, Alan Milburn) wants commissioning to mean is likely to vary on a bracingly frequent basis, if the continued existence of NHS England is anything to go by. (Which of course, it isn’t.)
A provider-led NHS
We are back to an explicitly provider-led NHS. HSJ‘s news seems to reveal provider trusts sharing chairs, chief executives or outright doing mergers and acquisitions on a weekly basis. This will have interesting consequences.
More than a decade after its publication, the 2014 David Dalton hypothesis of provider chains is almost happening by stealth. The Dalton Review is worth re-reading, as yet another example of reasonably sensible policy which got no real support. A sensible system would wonder why.
(This HPI piece from 2014 is also worth a re-read.)
How is this likely to meet Mr Streeting’s ‘neighbourhood health system’ vibes of the ‘triple shift’ from treatment to prevention and acute to community?
Expect some serious rhetorical contortions. Let’s hope that they don’t hurt too much.
Recommended and required reading
Concerning Financial Times piece on the current exodus of clinical researchers from the UK.
Fascinating piece on a woman who can smell Parkinsons disease: as my late father, a gas chromatographer would have instantly known, this means that the disease’s detection can almost certainly be automated.
Unsurprisingly, an employment tribunal has rules that a NHS trust chair is a worker of the organisation, and as such has the usual employment protections.
Work by The Observer and Democracy For Sale investigates fatalities in care involving a hi-tech patient monitoring system called Oxevision which has been rolled out in nearly half of mental health trusts across England.
A piece about AI that is not the most egregious hype? It can be done, as Samuel Hume shows us about AlphaFold.
Contrastingly, another weak Tony Blair Institute report hypes AI with no really good reason (apart from Larry Ellison of Oracle’s money).
Guardian comment piece on the need not to forget about improving patient safety in amid the new NHS redisorganisation, by Jeremy Hunt - who seems rather incurious about his longest-ever-tenure’s relationship to poor patient safety.
Ian Trenholm’s failed CQC ‘transformation’ cost £99 million. Ooops.
Michael Buchanan piece for BBC In Depth on the ongoing maternity safety scandal.
Conservative peer Lord Chadlington is again under investigation for pushing a business in which he was involved into the Covid19 VIP fast-lane.
The Times reports on a new study by LEK Consulting for SCI, which represents chemicals companies, which asserts that Britain’s life science sector has missed out on an estimated £15 billion a year over the past decade due to a decline in its international competitiveness.
Profile of Macmillan’s chief executive, who is having to make cuts.