Cowper’s Cut 268: Circular time

Health Secretary Steve Barclay has said the Royal College of Nursing should have waited before staging a 28-hour walkout, which is due to start at 8pm on Sunday evening.
— Sky News (@SkyNews) April 30, 2023
Read more: https://t.co/TO5LSmGPLu pic.twitter.com/GNm5o5g0u2
Oh good: a 'respect-off'
Secretary Of State For Health But Social Care Steve 'The Banker' Barclay and the RCN leader Pat Cullen started this week engaged in a 'respect-off'. It reminds me of that famous scene at the beginnning of The Godfather about 'showing no respect'.
God bless 'em. This 'respect-off' is sure to really move things forward. A quick reminder for The Banker about the Ipsos Veracity Index: nurses and doctors most trusted; politicians and journalists least trusted. Just saying.
As surely as night followed day, the NHS Staff Council voted to accept the Government's proffered pay deal. The majority in favour of settling on the electoral college was decisive: the body is understood to have voted by 27 to 17 in favour of the deal.
Adorably, Steve Barclay's sock-puppet and NHS Employers leader Danny Mortimer tried to 'both-sides' it with his response. Mmmmmmmmm. Danny's next conversations with the Royal College of Nursing and Unison (both of whom voted to reject the deal, and plan to continue industrial action) will be interesting.
There was some predictably poor analysis of what the vote for the deal means for industrial action, with a special prize going to The Guardian's heroically weakly-founded 'peace in our junior doctors' time' piece.
Our piece on the NHS pay agreement. Essentially, it's not all over, whatever the government may say. And whatever happens next, these strikes have been unprecedented - not even Thatcher compares https://t.co/oDetpNqxSh
— Georgia Banjo (@GeorgiaBanjo) May 2, 2023
The Economist avoided all of the obvious errors, with this thoughful review of today's NHS industrial relations landscape. It cited Dave Lyddon of Keele University, saying “the current Government has turned a lot of professionals into strikers”; and the Institute For Government's Stuart Hoddinott calling the Government's approach "unnecessarily confrontational”.
2/29 Lets start with the excellent pay graphs from the excellent @jburnmurdoch from the @FT published this week.
— Dr Tony Goldstone 💙 (@goldstone_tony) May 1, 2023
What do they show? They show we are NOT "all in this together" pic.twitter.com/UTQM9vX5YO
The BMA's Dr Tony Goldstone also helped to put what has happened to staff pay into striking context. Nope, not even sorry about the pun.
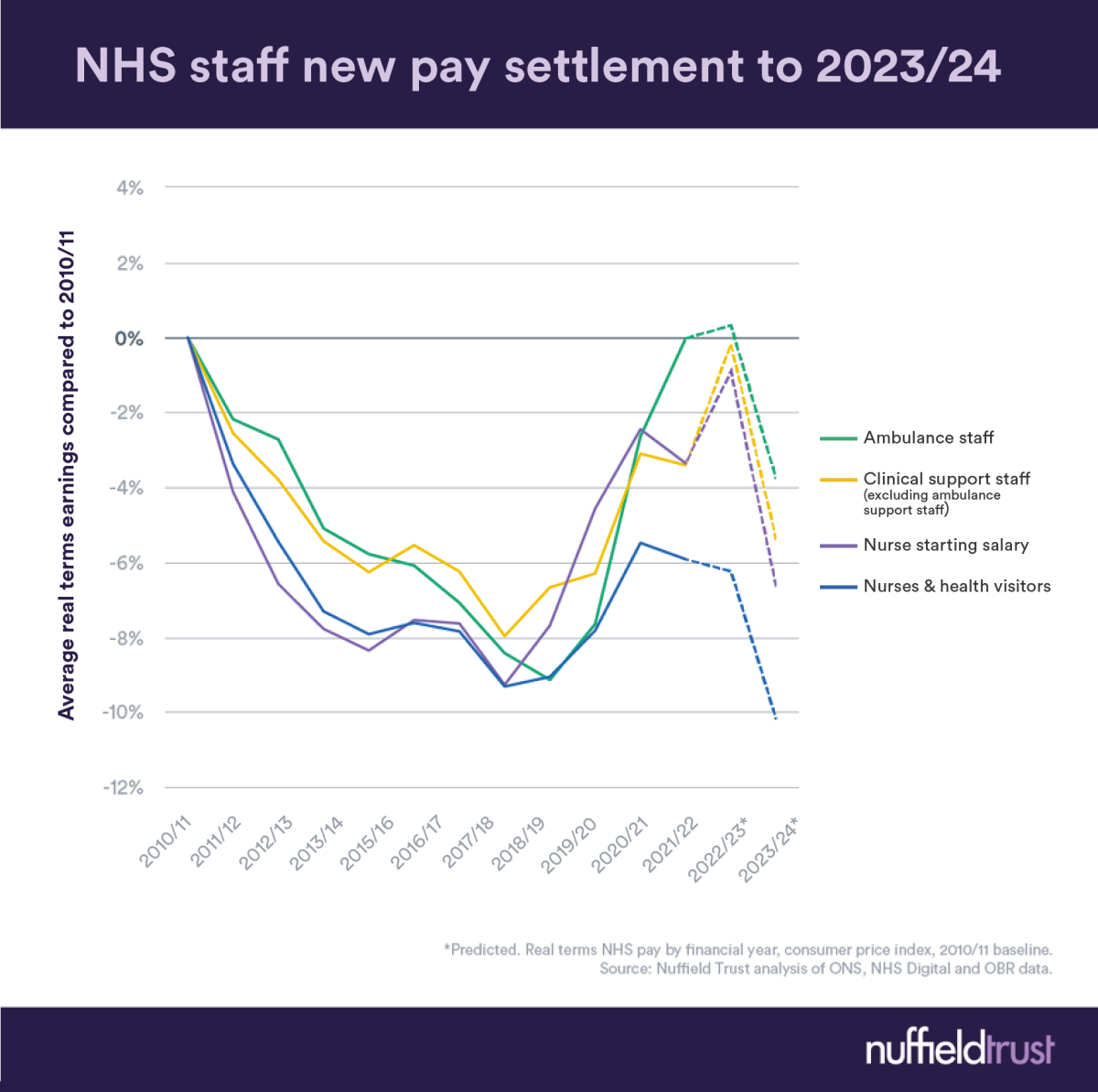
As Nuffield Trust analysis showed, this is not a great deal for which to settle.
“It is good day for NHS staff, it’s a good day for patients”
— BBC Politics (@BBCPolitics) May 2, 2023
Health Secretary Steve Barclay says there is an opportunity “for everyone to move forward together” after health unions backed an NHS pay deal for Englandhttps://t.co/6YoC48pNlZ pic.twitter.com/7CcZjYp4xm
Still, The Banker believes that this is an opportunity for "everyone to move forward together", and freedom of religious belief (however weakly-founded it may be) is important.
There's a point to be made about the strikers' motivations, which are not all financial or political. Many people know that as NHSE-seconded National Clinical Advisor in Emergency Preparedness Resilience and Response, Professor Kevin Fong did a considerable amount of work for NHS England going around the service talking to local organisations about their experiences of Covid.
I remain very struck by his retelling of a conversation that he'd had with a nurse manager.
This person told Kevin, "well, I know you're here on behalf of NHS England, and I'm sure that you're a very clever person, and I know that NHSE has lots of very clever people.
"And it's interesting to talk to you about how we're going to recover performance, but I really hope that all you clever people have got some plan to recover us - the staff - after this.
"Because we are broken. And I don't know how you're going to fix us.
"Because you're going to want us to fix the backlog, and there is no other workforce than us".
I don't think we can underplay, as the peer-reviewed research by Kevin and colleagues shows, the level of unprocessed trauma among NHS staff who were at the front line of the pandemic.
It varies widely from organisation to organisation, but my overall impression is that it doesn't feel as if recovering the Covid19 frontline workforce has been a top priority. Certainly when you look at those things put in for the pandemic to support staff (free parking, hot food provision, amenities in the workplace), they have mostly been removed. That's a major-league false economy.
I don't think it's a central motivation - but I suspect that if staff feel that insufficient or no effort has been made to recover them after the pandemic, then one part of the strikers' motivation (perhaps subconsciously) may be that they're recovering themselves - even at the cost of losing some pay.
Safety and systems
Two significant Health Service Journal stories this week touched on safety and systems. The first is about calls for a further delay to the launch of the Learning From Patient Safety Events database, which NHS Engroovement already delayed by six months, to September this year. This new system is due to replace the existing “national reporting and learning system”, which is thought to be outdated and at risk of failing.
HSJ "has heard concerns from several managers that an upgrade due in July to the RLDatix risk management system – which is used by the majority of trusts – will cause knock-on problems implementing LFPSE in September".
The second FOI-based story observes that despite their population health ambitions, just 18 of England’s 42 ICSs have in place the NHS Engroovement-mandated ICS-wide intelligence platform with a fully-linked longitudinal data-set to conduct planning, risk stratification and population health analysis.
This requirement is, HSJ notes, "a key part of NHSE’s digital aspirations for ICSs, which have been ordered to drive population health management across their patches so clinicians can intervene earlier in patients’ care and managers can improve NHS planning".
Local elections
The local election results do not predict the outcome of the next General Election, but they do make the political weather.
Pertinently, they change the local complexions (which can aggregate to regional effects) of the key local government functions of public health and social care, and a relatively strong showing for the Green Party.
As ever, Professor John Curtice's analysis is balanced and helpful.
'NHS@75'. Yes, really.
The NHS is a healthcare system, and not a person: as such, it doesn't have birthdays. The oncoming storm of simpering over its upcoming 75th anniversary of coming into existence is almost existentially emetic.
Still., it was charming to see the NHS Assembly gladly and of its own free will embarrass itself yet further by agreeing to be the facilitator of an 'NHS@75' publication about what the sector needs.
Health Service Journal reported its leaders' letter to NHS CEOs saying, "we know this is an extremely rapid process, at what is still an enormously busy time. We could have left it to the NHS Assembly and the representatives we have on it to give a view, but we believe that there is always time to engage. This is particularly true when things matter. The outcome of this process should help shape the future of the NHS. And your input matters.”
One must have a heart of stone not to laugh. This can, spiritually, join the immense list of NHS commissions, inquiries et al, whose output will test the 'heat-to-light' ratio to the outer limits of nanotechnology's detection ability.
Universal healthcare in any form is a wonderful thing. But if you want to provide decent quality care to all citizens at all times, and you need sufficient well trained, motivated and rewarded staff. After 75 years, the NHS does not even have a costed and committed workforce plan
— Dr Phil Hammond 💙 (@drphilhammond) May 3, 2023
A useful corrective to NHS sentimentality appeared in this first-rate long read by Richard Taunt of Kaleidescope Health And Care: it offers 'The Five Reasons Why The NHS Won’t Live To See 100'.
This is a serious analysis, and adds more meaningful challenge (and thus value) than I suspect we'll see out of any of the plethora of current NHS-75 commissions and reviews.
The private sector to the rescue? Erm, no
The Private Healthcare Information Network is a peerless source of information about private sector activity, and its latest data round-up is as useful as ever.
All is not rosy for the private sector, as the Laing Buisson coverage of Ramsay Healthcare's latest UK results shows. The company has an increase in the volume of business coming from the NHS, but they are being paid at tariff. The piece notes that "NHS tariff prices will need to grow alongside lower use of agency nurses for margin recovery": neither instinctively seems very likely.
Private providers are expanding in the UK: the Cleveland Clinic is opening a third site, and both HCA and Spire are also opening new facilities. Long waiting times are creating opportunities, but as more providers expand, the greater capacity created will not strengthen their case for significant additional premiums to the NHS tariff prices.
We can also anticipate some rebound in NHS hospitals doing additional waiting list activity, using NHS staff and NHS facilities in evenings and weekends, as the Budget's abolition of the lifetime pensions allowance makes this again worthwhile for senior staff.
This will probably limit the demand for more NHS-commissioned services.
It's worth reading this analysis for the Health Foundation of the independent sector's likely role and reach on helping deal with the NHS elective backlog.
Destroyed your notion of circular time
I was doing a dive into the archives of 'Cowper's Cut' when it appeared in HSJ, while I was trying to find out when I first referred to the Telegraph as the Boris Johnson Fanzine.
I was struck hard by looking over the last column of Cut's first run in HSJ. It noted that we had "no workforce plan, no capital/maintenance plan and no social care plan" ... at the end of April 2019.
We are now four years on, and not one of those key aspects is advanced, even one step.
Still, thank goodness for the Forty New (If Fictional) Hospitals.
Or is it 48?
It also set me to thinking about the only policy idea that I've ever had. Decentralising party political power over the NHS is evidently reversible, and indeed the reinvention of NHS Engroovement as the post-22 Act's 'more Matt Hancock' wholly-owned subsidiary of the Department For Health But Social Care has entirely reversed it.
Other freedoms have been reversed: Foundation Trust status no longer matters at all. And the NHS is evidently not better for these un-freedoms.
I suggest that the only irreversible approach to take the NHS out of party political ideology and timescales is to change its funding-setting via income taxation, and instead have it done as something along the BBC licence fee model. The money could be collected as presently, since it would be (as the licence fee is on television ownership) a tax to fund a universal service. But that should be the limit of the Treasury Munchkins' involvement: it would become an 'NHS Tax'.
Funding levels would be set by independent experts, who would produce and update plans on population health; provision; capital and maintenance; and workforce. Accountability, quality and redress would also be handled by an independent body, with representation from politicians, medics and citizens. Both organisations would meet in public and be required to be highly transparent, with minority reports parts of the system.
It'd need tight legal controls over assets, but in ways that will not freeze patterns of provision in the current model. Indeed, a new ownership format might enable longer-term approaches to capital funding. I'd be attracted to the idea of mutualising the NHS, because I think that ethos may be a good fit with universal healthcare.
The vast majority of spending would be devolved regionally, to ICSs (or whatever succeeds them), where public health staff would be developed to move into system leadership roles. National stuff should be what can best add value when done once for all: sharing best practice; high-spend procurements; data and safety recording and reporting; workforce training standards and reforms; national-level investment and disinvestment programmes; pandemic preparedness (ahem).
I'd be fascinated to hear readers' thoughts about why this couldn't work, and of what else it would need.
The Alan comeuppance
Ex-Health Secretary, former Conservative MP and current cryptocurrency shill Matt Hancock was briefly back in the news this week, as the Register of Members' Interests revealed his having charged 'Good Morning Britain' £10,000 for an interview back in January.
GMB are, of course, absolute mugs to have paid The People's Partridge; but it's a sign of the 'politician self-identifying as celebrity' culture that has so royally reamed our politics.
Recommended and required reading
Fascinating FT long read about the adoption of innovative medicines in the NHS, looking particularly at inclisiran and the Grail trials.
Centre For Policy Studies boss Robert Colvile's latest Sunday Times column is a decent canter around some of the NHS's big problems.
Nuffield Trust's new report, 'Building a resilient social care system in England: What can be learnt from the first wave of Covid-19?'